
Item 1
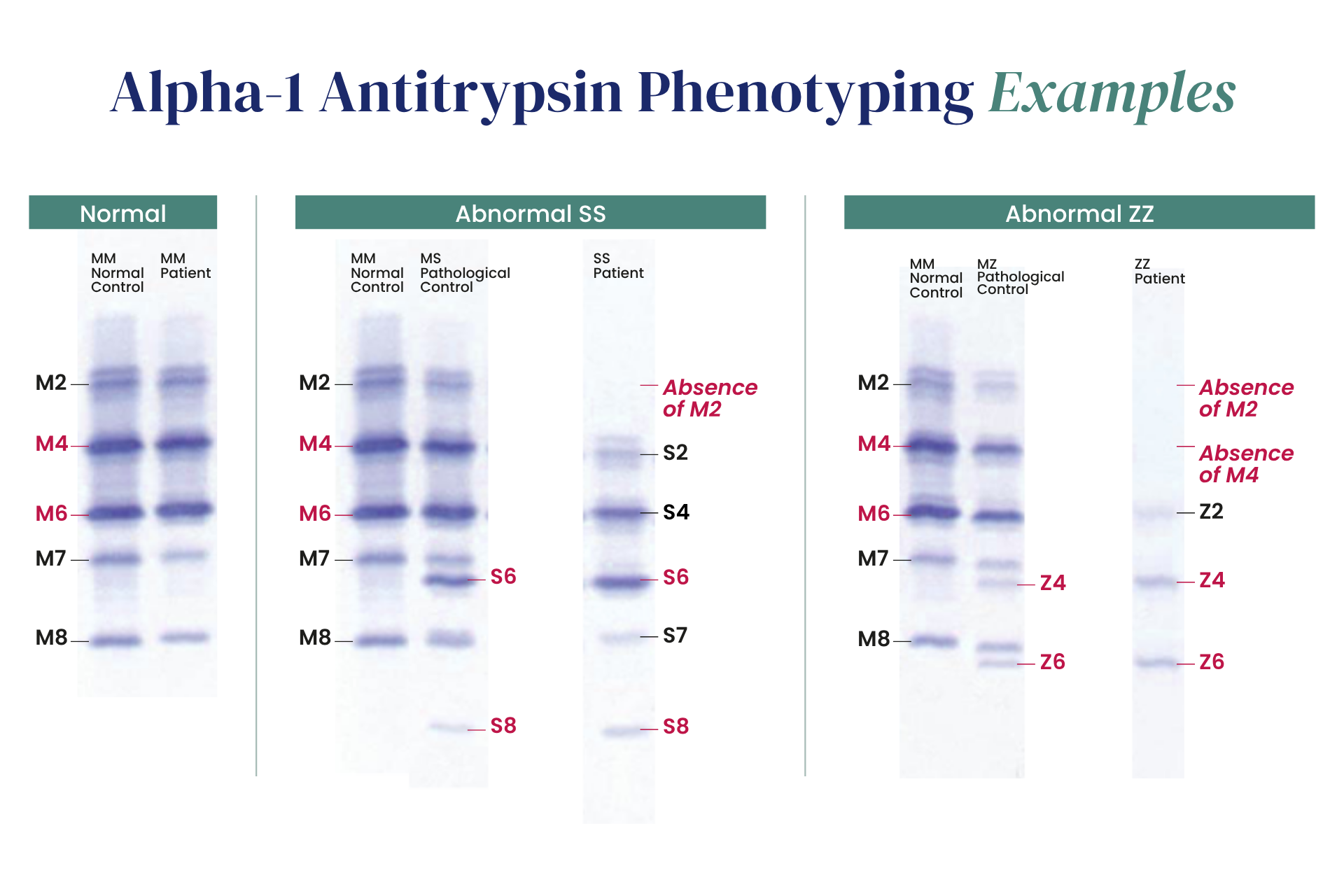
Pulmonary manifestations of Alpha‑1 Antitrypsin Deficiency (AATD) typically appear after the age of 40, whereas hepatic involvement can occur much earlier, including in childhood. Early identification is essential, as disease progression can be slowed through timely therapy and by reducing exposure to aggravating factors. Identifying individuals at risk for AATD‑related lung and liver damage and enrolling them promptly in appropriate management programs is therefore critical. Although clinical guidelines recommend testing all patients with COPD or unexplained bronchiectasis for AATD, up to 90% of individuals with severe deficiency remain undiagnosed, often for years after symptom onset. Several diagnostic methods are available. The most widely used is protein phenotyping by IsoElectric Focusing (IEF). AAT concentrations can also be measured by nephelometry or immunoturbidimetry, but levels may fluctuate due to unrelated inflammatory or physiological conditions, which can obscure true deficiency. Genotyping assays can detect common deficiency alleles such as S and Z, but may miss other pathogenic variants, leaving some at‑risk individuals unidentified.

